Health, Safety and Environment Bulletin June 2018
Fall from Height – Fatal Injuries – FACTUAL INFORMATION
Vessel
MV Pompano is an 88,845 GT bulk carrier built in 2006 and registered in Malta. Pompano had an overall length of 289 m and a moulded depth of 45.00m – the capesize bulk carrier was fitted with 9 steel cargo holds with a total grain capacity of 193,134 mt and the vessel was strengthened for heavy cargoes.
Crew
Pompano’s Minimum Safe Manning Certificate stipulated a crew of 17. At the time of the accident, the vessel had a crew complement of 19. All crew members were Filipino nationals, except for the master who was Greek.
The fatally injured third engineer was 35 years old. He had spent the previous five years at sea, three of which with the current Company. He had been serving as third engineer for a month; prior to that, he was an oiler for four months and a fourth engineer for two years.
Repairs inside Cargo Hold No. 3
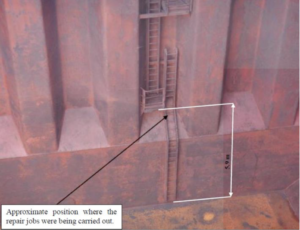
The crew members had been tasked to repair the damaged cargo hold access ladder platform’s safety rails. The repair job involved the removal and replacement of several safety rail sections, necessitating fabrication and the use of gas cutting and arc welding equipment.
Environment
On the day of the accident, the weather was clear with calm seas. Logbook records indicated that the Westerly wind was force 2 and the air temperature was 32 °C. The sea temperature was recorded at 30 °C.

Narrative
On 08 April 2017, the chief engineer was informed by the master that some lengths of railing on the lower platform of the straight ladder on the forward bulkhead of cargo hold no. 3 required repairs. The chief engineer verified the availably of material on board and confirmed to the master that the job could be done.
The ‘Hot Work’ and ‘Work Aloft’ permits had been completed and approved. The chief mate instructed the bosun and the third engineer to prepare the site with materials and tools while the chief engineer proceeded down to the cargo hold no. 3 to evaluate the job. After making the preparatory work, the chief engineer suggested to continue the work after lunch.
After lunch, the chief engineer, along with the third engineer and one of the OS, proceeded to cargo hold no. 3 to commence the repairs. The chief engineer and third engineer went inside the cargo hold to take measurements and eventually start the job. The third engineer was wearing a safety belt and a safety helmet, in addition to welding PPE. The repairs had to be carried out in way of the lower platform, which was about 5.9 m above the tank top (Figure 2).
The third engineer started to cut the damaged rails. In the meantime, one of the OS went down inside the cargo hold to assist him. Later on, the chief engineer and the OS went up to the main deck to heave up the damaged rails cut by the third engineer. After which, the crew members went back to the accommodation for a rest break.
After the break, the third engineer and the OS went back inside the cargo hold, while the chief engineer went to the engine-room to prepare the angle bars for fabrication. Once he finished with the angle bars, he carried them to the cargo hold. He lowered the angle bars into the cargo hold to the OS, which he passed over to the third engineer.
The chief engineer could make visual contact with the third engineer on the tank top, as well as when he was climbing the ladder to reach the lower platform to weld the angle bars. The chief engineer went again back to the engine-room to cut the flat bars and pipes. On his way to the engine-room, he saw the fourth engineer and asked him to assist in the cutting of the flat bars and pipes. Once finished, the fourth engineer was instructed to carry the material to the cargo hold while the chief engineer remained to secure the long pipes back to their place in the steering gear flat.
At about 1705, while the third engineer was shifting his position to climb down the ladder, he fell down to the tank top. Immediately, all available hands rendered assistance. The OS raised the alarm and the second mate administered first aid.
The injured crew member was observed to bleed profusely and was also unresponsive. The local VTS was contacted to report the emergency and to request urgent assistance.
Although the second mate and other crew members continued to give medical assistance, the third engineer could not be resuscitated. At 1845 and 1852, paramedics and a doctor arrived on board respectively. At 1908, the doctor pronounced the third engineer dead, noting also a very severe head injury at back of his head.
ANALYSIS
This marine safety investigation is to determine and circumstances and safety factors of the accident as a basis for making recommendations and to prevent recurrence.
Immediate cause of the accident
It was established that the third engineer had fell off from the sloping section of the forward cargo hold access ladder, just below the lower most platform to the cargo hold tank top.
The following were also investigated but none established evidence that attributed to the accident:
- Drug and alcohol consumption
- Fatigue
- Design of the ladder
- Loss of balance due to abrupt vessel movement
- Physiological condition of the fatally injured crew member
Besides which, the following evident to be the main reasons for the accident:
Personal protective equipment – missing protective barrier systems
- The safety helmet (Figure 4) was old, stained by oil and appeared to be less than adequate upkeep. The plastic band was also rigid and not elastic. Notwithstanding this, the safety helmet would highly probably not have prevented the head injuries sustained by the third engineer.
- A safety belt (Figure 5) was used though a five-point fall arrestor was available onboard. It is in poor condition with a corroded belt buckle, rigid belt lanyard and a defective safety clip.



Safety Management System Procedures not followed
- No evidence of toolbox meetings prior to the repair
- Wrong risk assessment template was used – the template wasfor work aloft carried out on the monkey bridge mast
No evidence to suggest that another officer had been appointed to oversee the work when the chief engineer was engaged in the engine-room workshop
Perception and acceptance of risk
The safety investigation was of the view that risk had not been accepted blindly by the crew members. Risk assessment (albeit the wrong one) and work permits indicated a perception of risks well under their control and did not require extraordinary efforts to mitigate. Hence, there is possibility that a perceived ‘safe’ task could have led to acceptance of higher risks.
This also reflected the importance of toolbox meetings and detailed risk assessments. Risk assessments and toolbox meetings are ways of making the boundaries of system performance more visible and would have enabled the crew members to address the identified risks.
Actions by the third engineer on his way down the ladder
The members were aware of the risks involved and which, out of necessity, they had accepted. Yet again, there were a number of influential factors which would have played a crucial role on whether risk was acceptable or not, and which were applicable in this case. Risk perception is actually influenced by cultural, social, and psychological contexts.
The fact that the fatally injured crew member selected to release his safety belt from its anchor point is actually a risk which he had chosen; on the basis that in reality, it was the best alternative available to him. Similarly, risk tends to be more accepted if it is perceived to be under the control of the person. Therefore, if the third engineer did perceive that the situation was under control (even because this was not a complex task to complete), then his perception of risk would have been influenced towards accepting the risk of releasing the safety belt from its anchor point.
Perception of control, however, does not mean actual control and more often than not, it is more of an over-estimation of the capabilities of the person to control the situation.
SAFETY ACTIONS TAKEN DURING THE COURSE OF THE SAFETY INVESTIGATION
During the course of the safety investigation, the Company:
-
- Conducted a fleet wide review of safety harnesses, with eitherupgrading or replacements carried out where necessary;
- Distributed a fleet safety circular, highlighting the issues of risk/hazard assessment, rigour to work permit systems andappropriateness / condition of PPE;
- Painted the top of the lower stool yellow to highlight thechange in the ladder’s inclination and distinguish it from thecargo hold tank top;
- Reviewed its ISM internal audit and marine inspections’ scopeand process in terms of rigour, objectivity and frequency;
- Amended the SMS in order to further formalise the work inside cargo holds (in terms of height and hot work). Working procedures have been added, including provisions for risk assessments, work permit and general HSE considerations.Visual aids have been included;
- Reviewed and updated the risk assessment template;
- Briefed all crew members on this accident;
- Reviewed its senior officers’ familiarisation process, to includetopics on risk assessments and safety culture in general;
- Issued safety bulletins on this accident.
The IMO has recognized the threat of cyber-attacks in the marine industry and will require considering cyber risk management as a part of ship operators’ safety management system. A cyber security assessment will be required which should be done no later than the first annual inspection of the company’s Document of Compliance after 1 January 2021.
Bridge Systems and ECDIS
Amongst the many systems that must be considered within this assessment is the bridge navigation equipment. Equipment such as ECDIS that receives frequent updates to its chart catalogue and its software make it high risk. It may also be possible for anyone on the bridge to plug their own device into the ECDIS via a USB port.
How is ECDIS Vulnerable?
Ship operators will need to initially identify any vulnerability to their vessel’s cyber security. In the case of ECDIS this can include: Interfaces with shore side systems. This type of interface is often used to conduct software updates remotely. The ECDIS can also be interconnected with other navigation systems, such as GNSS and ARPA. This can make the system vulnerable to a virus spread between platforms. Control of removable media such as USB drives and CD which are commonly used on ECDIS to install updates to the ENC’s, the permit files and software.
Any removable media sources must be checked to ensure they are free from malware. Any breach of ECDIS security could result in ECDIS sensor data being manipulated with unreliable information displayed to the officer of the watch. It could even mean a total loss of the ECDIS and any equipment on its associated network.
Assesment and Detection
The cyber security assessment identifies the likelihood and impact of a potential breach, and put in place measures in the ship’s management system to ensure these threats do not become a reality. The measures put in place are to ensure that any threats are detected before they become an issue. For example, if an update to the ECDIS means using removable media, such as a USB drive, then checks on the content should be run prior to using the drive. Access to the ECDIS to conduct updates should be limited to as few people as possible as a way of protecting equipment.
When You’ve found a Threat!
The responses to a detected threat should be included in the procedures put in place to protect the vessel. The IMO Guidelines on cyber security advise that a team should be established, and a recovery plan put in place, to take the correct steps to restore systems such as ECDIS to a safe working condition.
Help is at Hand
All activity on the ECDIS should be logged and accurate records maintained. The following steps are outlined – the crew should take when updating their ECDIS:
-
-
- Identify Threats – what is the source of the threat?
- Protect – what can happen as a result of the threat?
- Detect – how will you find a potential threat?
- Respond – what steps will be taken to prevent the threat?
- Recover – how to respond in the event of a cyber security breach?The ADMIRALTY ENC and ECDIS Maintenance Record (NP133C) is designed to help mariners demonstrate compliance with IMO regulations during Port State Control inspections, with easy-to-use checklists and templates to record ECDIS annual performance checks and software maintenance.
-
(Source: North P&I Club)
What happened?
During a vessel dry dock, smoke was observed coming from a forepeak store, which was also accessible from the mess room. Expired hand flare pyrotechnics, boxed and packed up for landing ashore, had been accidentally activated by yard personnel on board for cleaning and chipping the chain locker.
The alarm was raised and the necessary steps were taken for the safety of the crew and yard personnel.
What went wrong? What were the causes?
Procedures were not followed:
-
-
- the third-party contractor personnel had been briefed regarding thecompany’s safety management system (SMS) but this incident stilltook place
- where third-party personnel are working, the area should bethoroughly checked for any unsafe practices that can take place.What actions were taken? What lessons were learned?
-
- It was noted that since the forepeak store was also a provision store with access from the mess room, the risk of theft or pilferage could not be neglected;
- The expired pyrotechnics were sent back to the approved vendor.
-
(Source: IMCA Safety Flashes)
Lessons Learnt: Oil Spill due to Failure of Cargo

A tanker was fixed to load a petroleum product cargo at an offshore anchorage by ship to ship transfer (STS). After making fast alongside the storage vessel, cargo tanks were inspected and pre-loading checklists completed which included agreement on the maximum cargo transfer rate. A flexible cargo hose supplied by the STS service provider was connected between the respective vessels manifolds. During transfer operations, the cargo hose ruptured near the receiving vessel’s manifold, causing oil to spray on deck and overboard. The crew responded immediately by raising the alarm, instructing the storage vessel to stop the transfer and by taking prompt action to confine and collect oil spillage on deck. After clean-up operations and the subsequent investigation were completed, the hose was replaced and operations resumed.
Analysis
Only a very small quantity of oil was released into the sea, mainly due to the quick and effective response of the crew. The investigation into the incident concluded that the failure of the hose was related to its condition as there was no evidence that the agreed pumping rate or pressure in the system was exceeded. Markings on the hose indicated that it was last pressure tested more than two years before the incident and no valid certificate of inspection and test could be produced on demand. In this case, responsibility for confirming the hoses were fit for the intended service and properly certificated rested with the STS Service provider. However, the crew should carefully inspect transfer hoses as far as safely accessible and request access to the hose documentation, cross checking that identification markings match up and protesting any defects or anomalies. Industry guidelines require that periodic tests of hoses are undertaken at intervals not exceeding 12 months.
Lessons Learnt
-
-
- Ship to Ship transfer operations must be performed taking into consideration the requirements of the vessel STS operations plan, MARPOL regulations for the prevention of pollution during transfer of oil at Sea, the Ship to Ship Transfer Guide and the vessel Safety Management System
- Cargo transfer hoses should be fit for purpose and provided with valid records of test and inspection
- Any evidence of deficient or non-compliant transfer hoses should be protested and thereafter investigated / rectified by the responsible party
-
This incident demonstrates the vital importance of the crew keeping a vigilant deck watch during transfer operations and in responding rapidly to contain a spill in accordance with drilled procedures
(Source: UK P&I Club)
We all encounter stressful events in our personal, professional or social life. It is important to remember that not all stress is negative, some stress is positive, motivating us to maximise our productivity and creativity.
In contrast,‘distress’ is negative stress, which,“is evident when a person perceives himself as lacking the ability or the resources to control a stressful situation” (Selye, 1976).
Stress is defined as,“a negative emotional experience accompanied by physiological, cognitive and behavioural changes and responses aimed to reduce or change the stressful event or effects of it” (Baum, 1990). How well we cope with stress is mediated by our appraisal of the stressor and the resources available to deal effectively with the stressor.
Unequivocally, seafaring is a strenuous occupation, and seafarers are exposed to an increased number of work related stressors: fatigue, long hours, monotony, noise, vibration, temperature changes, a multinational environment, limited recreation, isolation, long periods away from home. In other words:“Factors that may produce an imbalance between work demands and personal resources leading to a decline in physical and psychological health and an increased risk for accidents and injuries”. (Carotenuto, et al, 2012).
Most seafarers can suffer from moderate to high stress that can lead to a vicious cycle of unhealthy behaviours that are difficult to escape: sleep disturbance, unhealthy eating and weight gain, causing mental and physical ailments.
Physical symptoms of stress include: anger, irritability, fatigue, nervousness, lack of interest or motivation, anxiety, sadness, muscular tension, faintness, dizziness, headaches, indigestion, stomach aches, appetite changes, erectile dysfunction, change in sex drive and teeth grinding.
Tips for dealing with stress
-
-
- Identify the strengths and skills that increase your confidence. Think of a survival resource that helped you cope with a stressful experience in the past.
- Assess, recognise and develop your creative resources: talents, traits, skills or competencies.What are your resources? Optimism, humour or flexibility?
- Evaluate your resources. Are they internal or external? Internal resources refer to personality traits like humour, optimism, courage, flexibility, spiritual connections or accountability. External resources can be hobbies, activities, team or religious associations or social support.
- Use cognitive reappraisal when evaluating a negative event. Notice the negative thinking causing you emotional tension. It is mostly how we interpret events that evokes negative emotions.
- Engage and interact with other people onboard. Do not isolate yourself – become interested in learning and engaging with your team mates.
- Establish an open communication channel with somebody you trust to discuss your difficulties or concerns.
- Do not let negative emotions overtake you.When something bothers you, address it immediately – don’t turn it into rage, sadness or resentment.
- Be realistic about your expectations.
- Be accountable for your actions.
- Develop a healthy lifestyle by eating a balanced diet,maintaining asleep and rest schedule, exercising regularly and partaking inrecreational activities.
- Keep a diary to note your thoughts and feelings.
- Practice mindfulness and relaxation techniques.
-
(Source: UK P&I Club)
The Health and Safety Bulletin is a quarterly publication of Western Shipping Pte. Ltd. – Singapore.
The contents of the newsletter are compiled in good faith to promote Safety, health and environment protection. We are deeply indebted to all the sources, which are not individually mentioned.